Is it 100% possible to rule out dislocation with an AP shoulder? Most Radiologists would tell you that it rarely requires anything more than an AP view, but occasionally, you will need to get an additional "Y" view shoulder. It is possible to have a dislocation either anteriorly (more common) or posteriorly and have very little difference of appearance than a normal AP radiograph if one view is taken.
This is another way to obtain a "Y" view shoulder with the patient lying supine: Make sure the patient is perfectly flat with no rotation to either side. Place a 10 x 12 cassette crosswise under the patient's back. The center of the cassette should be directly over the midsagittal plane. I like to place the top of the cassette about 1 inch above the palpable acromion process (don't worry - the tube angulation will project the scapula over the film).

Angle your central ray 45 degrees to enter the patient's affected side at the surgical neck of the humerus and make sure to collimate. Just as in the trauma oblique c-spine technique (if using a grid), make sure that the cassette orientation is crosswise to avoid grid cutoff. Place the patient's affected hand on top of the abdomen if possible. If you are reluctant to collimate, just remember that the proximal humerus should superimpose the scapula... this is probably easier to line up than the standing PA oblique method - cone in to the humerus. This should be done on suspended respiration, and as a general rule of thumb, three times the mAs from the AP projection should be employed.
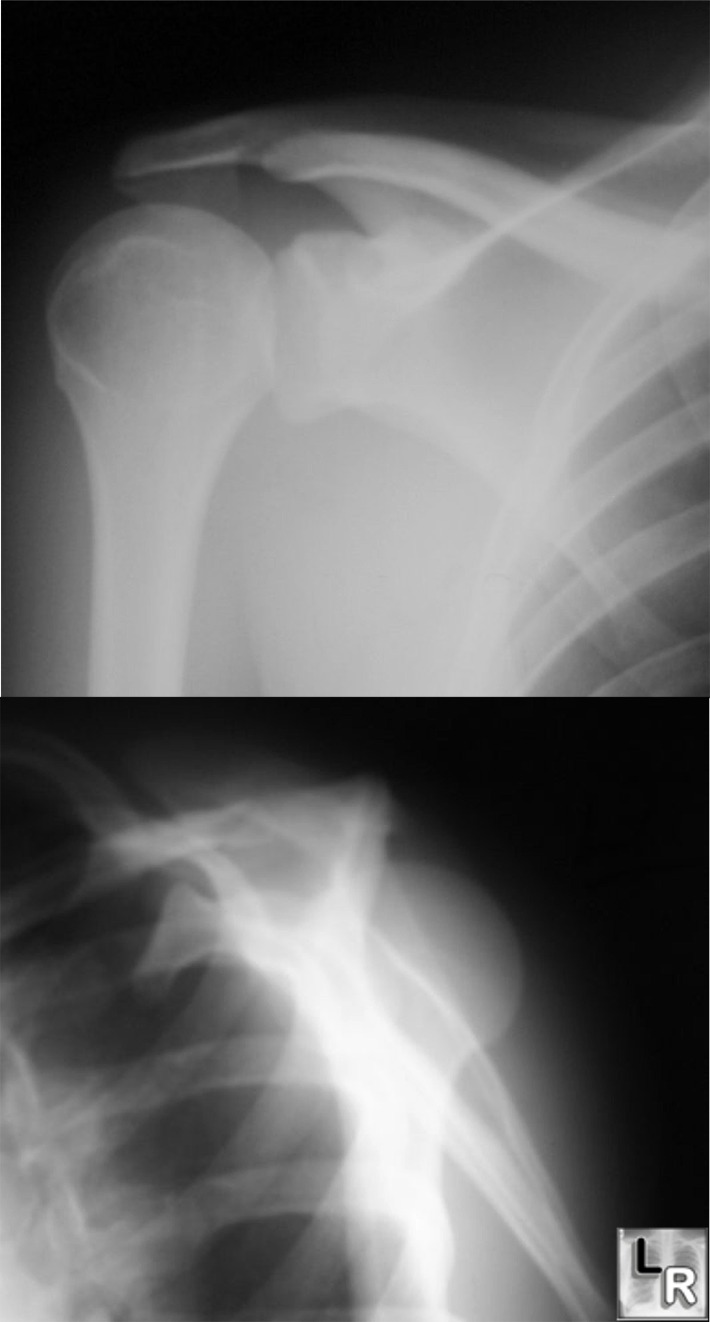
The following x-rays (courtesy of Learning Radiology) show a posterior dislocation... difficult to diagnose from AP view, but fairly easy to identify on the "Y" view.
After you have performed this view, you'll notice quite a bit of elongation. Every once in a while, I will get a request for a repeat without elongation from either the ER physician or the radiologist. If you can get cervical collar clearance, you can still do an AP projection for this view while supine. I find that if you place a 45 degree sponge behind the patient's shoulders (as you might do with an oblique L-spine view), the Y shows up wonderfully as long as the patient's humerus remains parallel to the body.



Hi Jeremy,
ReplyDeleteI really liked the scap-y explanation and picture. I have been having a heck of a time getting that one right for some reason. We do scap-ys as routine for a trauma or non-trauma shoulder x-ray, so I really want to get them right. Keep up the good work with the site. Its all very interesting and helpful.
Dustin (former student of yours in AZ)
Hi Jeremy,
ReplyDeleteI really liked the scap-y explanation and picture. I have been having a heck of a time getting that one right for some reason. We do scap-ys as routine for a trauma or non-trauma shoulder x-ray, so I really want to get them right. Keep up the good work with the site. Its all very interesting and helpful.
Dustin (former student of yours in AZ)
Thanks Dustin... I've always struggled with this view. Everybody has at least one that they have trouble with. I'm glad you like the blog - I'm working on some more topics, but might not have another post for a few days at least. I wish I could be around to hear some of your class's stories! Keep up the good work.
ReplyDeleteThanks Dustin... I've always struggled with this view. Everybody has at least one that they have trouble with. I'm glad you like the blog - I'm working on some more topics, but might not have another post for a few days at least. I wish I could be around to hear some of your class's stories! Keep up the good work.
ReplyDeletehi!
ReplyDeleteas a student just finishing up his first year, for me the scap-y was one of the most difficult views to perfect. i finally had to recrack open my cross-sectional anatomy book to get a general idea of proper angulation to have the cr parallel to the scapula. i'll definitely give your view a shot next time i have a rotation in the ER. thanks!
hi!
ReplyDeleteas a student just finishing up his first year, for me the scap-y was one of the most difficult views to perfect. i finally had to recrack open my cross-sectional anatomy book to get a general idea of proper angulation to have the cr parallel to the scapula. i'll definitely give your view a shot next time i have a rotation in the ER. thanks!
hi! I'm Nelson from the philippines, a Radiologic Technologist from Philippine Orthopedic Center, a specialty hospital of the bone, I've been in my profession for about more than 20 years. presently assigned at the emergency x-ray section. I just viewed and read your Y scapular. Actually its my first time to see that kind of positioning. Here doing scapular y view has two options, if patient is said to be had a multiple injury we just elevate the injured side for about 45 degrees body position with the tube is perpendiculary directed to the film and we can clearly demonstrate the y view, and the other one is taken in standing position this for cooperative patient. but when I read your technique I was somewhat amazed. for sure I will try to apply your technique soon. thank you.
ReplyDeleteThanks Nelson... I would prefer your two mentioned ways of performing the Y-view because it will eliminate elongation, but this one seems to get the job done if the patient cannot be taken off a backboard or moved and you want to investigate for dislocation. Let me know how it works for you... the trickiest part is lining up the image receptor.
ReplyDelete