I know I have posted about this topics before, but I would like to stay on this soap box for a while because I know that education still needs to occur regarding dose reduction techniques using CR and DR equipment. Over the past several years since I began writing here, a lot of improvements have been made in the materials used and sensitivity of our digital radiography equipment, which reduces radiation dose significantly. For some reason, either technology has progressed far faster than the continuing education of our peers, or technologists are resisting the pace of change occurring with imaging technology, and grids are not being used as they should.


In 2008, I had the pleasure of attending a workshop on digital radiography with lecturers Barry Burns, James Barba, and Andrew Woodward at the University of North Carolina. After putting to practice the principles taught there, everything has held true over the last 5 years. I'm going to show you two recent x-rays of the same patient which support the information presented. The first was done without a grid and the second with a grid. Keep in mind that the patient was just over 100 lbs, so very small in relationship to the average patient size.

85 kVp 5 mAs, non-grid, optimum exposure indicator
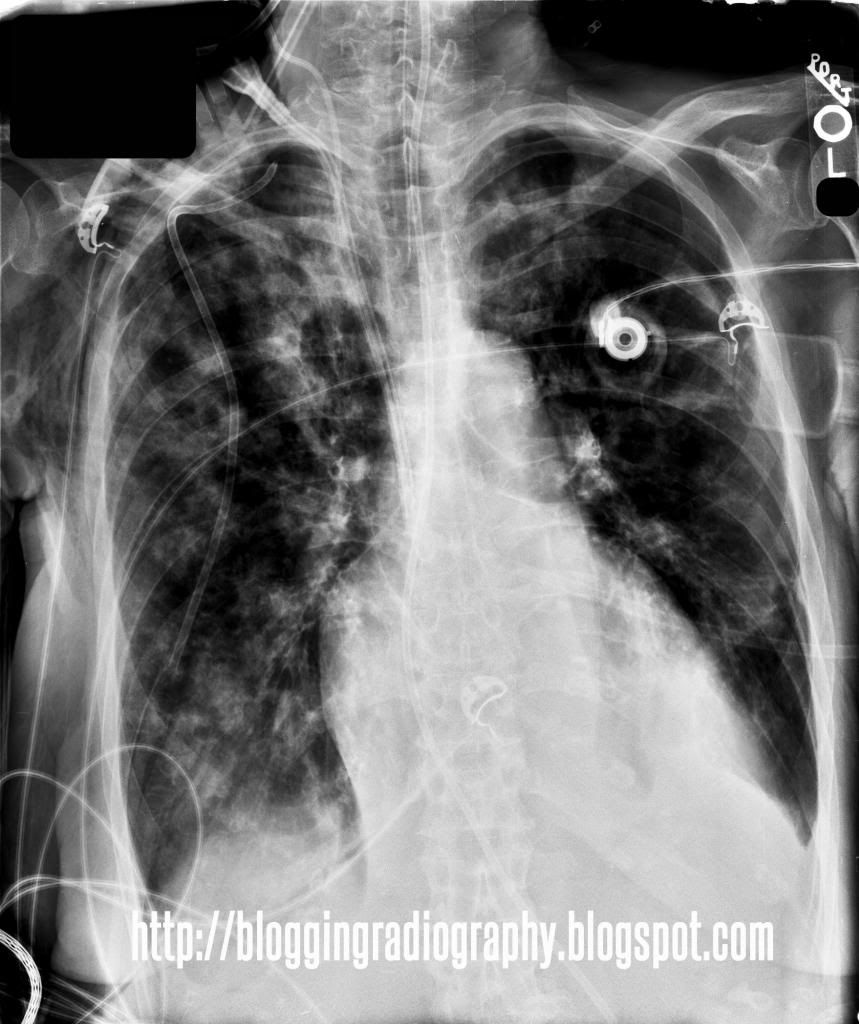
120 kVp 3.2 mAs, 8:1 grid, optimum exposure indicator
Both of these images were taken using some very aged FUJI CR image plates (see image plate chipping damage on top of the images - I hear they're being replaced). They were taken by different technologists within the same week. The non-grid film was taken in an ICU bed prior to portacath insertion, while the gridded image was obviously taken after.
Advantages:
Advantages:
- Higher quality beam = more uniformly penetrating. You can not only see thoracic spine through the mediastinum, but there is also better visualization of the central line, chest tube and NG tube. It is difficult to see below the diaphragm or even through the mediastinum at lower kVp without a grid.
- Higher kVp and lower mAs = lower patient dose. With higher kVp, the entrance skin exposure is lower because there is more energy behind the photons pushing them through the patient anatomy. The lower mAs value speaks for itself as mAs is directly proportional to intensity.
Disadvantages (trying hard to come up with any):
- Some technologists struggle with grid cutoff on portable chest exams. Strategies for reducing cutoff include perpendicular beam, using lengthwise orientation when possible, or utilizing a short-dimension grid. Sliding the patient up in the bed prior to sitting the head of the bed up is essential (read "Lordotic Much?" at the end of this post). In other words, there is less positioning latitude.
In my opinion, there is a clear choice. When we can prioritize patient dose while improving image quality, why would anyone want to do otherwise? Of course, I'm here to learn as well as to publish my opinion, so I welcome any comments, suggestions, criticism, etc.
Other related posts:


thanks very much for your large information .and knowledge full description . i think it is sus a topi that many kinds of people face many problem. thanks for this.
ReplyDeleteInformation visualization Low
thanks very much for your large information .and knowledge full description . i think it is sus a topi that many kinds of people face many problem. thanks for this.
ReplyDeleteInformation visualization Low